Ankle sprains are one of the most common injuries to occur. Women are at greater risk, as are children and adolescents and those that play indoor or court sports such as basketball or netball. This probably comes as no surprise, what may surprise you is how the management of these injuries has progressed away from the old ‘ice and rest’. At GV Sportscare our Shepparton Podiatrist and Physiotherapists are experts in ankle sprains, having worked on football teams, netball teams and closely with foot and ankle surgeons. Read on to learn about some of the myths behind ankle sprains!
Myth #1: Crutches are essential to faster recovery
 Most people are surprised to find that their physio or podiatrist is very keen to get them off crutches ASAP. In severe ankle sprains or suspected fractures, crutches are required, however in the mild to moderate ankle sprain crutches will actually slow down your recovery. Crutches reduce the weightbearing through the joint (which is a good thing if there is too much pain and damage). However in a mild to moderate injury it is unnecessary and will cause you to lose movement and strength, which you will need to work harder to regain as part of your rehab. Your Shepparton Physio or Podiatrist are able to assess your injury and guide you as to whether or not crutches are required and work with you to wean you off them!
Most people are surprised to find that their physio or podiatrist is very keen to get them off crutches ASAP. In severe ankle sprains or suspected fractures, crutches are required, however in the mild to moderate ankle sprain crutches will actually slow down your recovery. Crutches reduce the weightbearing through the joint (which is a good thing if there is too much pain and damage). However in a mild to moderate injury it is unnecessary and will cause you to lose movement and strength, which you will need to work harder to regain as part of your rehab. Your Shepparton Physio or Podiatrist are able to assess your injury and guide you as to whether or not crutches are required and work with you to wean you off them!
Myth #2: I need to see a Shepparton GP before seeing a Physio or Podiatrist
Podiatrists and Physios are well trained in assessing and treating ankle sprains and can refer you for any relevant scans such as x-ray and MRI, if required. We have specialist tests we can perform and provide you with taping or ankle supports on the spot, should you need them. We can also begin your rehab process of exercises from your very first session. This is very important as early movement and strength work can fasten your recovery or return to sport. So in summary within one physio or podiatry session we can diagnose or send for scans, tape or fit a brace or crutches (if necessary) and start you on exercises, all with the goal of return to activity or sport ASAP!
Myth #3: My x-ray is clear so I am unlikely to have sustained a severe injury
X-ray is used to clear fractures. Some fractures are too small to be picked up on x-ray and require a CT or MRI. This can include what we call an OCD (osteochondral defect), where a small piece of bone/cartilage has chipped off and can be sitting somewhere it shouldn’t. These often need to be removed as they can push and wear away on the cartilage where they shouldn’t.
X-ray is always used when the person is unable to weightbear as a precaution to check for fracture (we are actually required to x-ray if you cannot weightbear). This is even more important in the child or adolescent as they are more likely to fracture. This is because in children the bones aren’t fully fused as in adult bones and therefore the bones are more susceptible to fracture.

X-ray also can’t tell you how severe your ligamentous injury is. Sometimes you can see a syndesmosis injury (when the tibia and fibula have separated due to damage to the ligaments between them) on x-ray. However ligamentous injuries can often take much longer to recover from and have long lasting effects on your ankle stability.
Myth #4: I need to wait a few days before being seen by a Physio or Podiatrist
 The sooner you can be seen by your Podiatrist or Physio the better. When we waste a few days with the wrong management you are slowing down your recovery. Most people think injuries are a time based recovery, ie I have sustained a grade one ankle sprain therefore I will be back to sport in 2 weeks. This is partly true, injuries require healing and that takes time. However from our point of view your return to sport or activity is mostly based on ticking off certain criteria. For example can you raise onto your toes, can you stand on one leg, can you hop, can you run, etc. If you can’t do these things it doesn’t matter if your two weeks has passed, you are still not ready to return to activity. We then base our rehab on what you can and can’t do and aim to progress you on as quickly as possible.
The sooner you can be seen by your Podiatrist or Physio the better. When we waste a few days with the wrong management you are slowing down your recovery. Most people think injuries are a time based recovery, ie I have sustained a grade one ankle sprain therefore I will be back to sport in 2 weeks. This is partly true, injuries require healing and that takes time. However from our point of view your return to sport or activity is mostly based on ticking off certain criteria. For example can you raise onto your toes, can you stand on one leg, can you hop, can you run, etc. If you can’t do these things it doesn’t matter if your two weeks has passed, you are still not ready to return to activity. We then base our rehab on what you can and can’t do and aim to progress you on as quickly as possible.
Myth #5: Icing and anti inflammatories are the best treatment for swelling
Ice
Icing is great to help numb the area and therefore relieve pain. However compression and elevation are far more important to help decrease your inflammation. Swelling in the ankle is particularly hard to get rid of due to gravity, as the fluid has no chance to escape the area. Compression helps to increase the pressure and essentially push the fluid out and elevation allows gravity to assist the swelling to move out of the area. There is actually very limited scientific research to prove that icing has much effect on swelling!

Swelling management: you can see the effects of a compression bandage and elevation on the swelling of this ankle.
Anti inflammatories
 In the first 48-72 hours of your injury it is recommended to avoid anti inflammatories such as ibuprofen (Nurofen) and Voltaren. This is because the inflammation that occurs is your body’s response to injury and it actually brings special healing cells to the area that are beneficial for your recovery. This includes cells that remove debris and other cells that repair tissue. Therefore this early inflammation is actually a GOOD thing and taking anti inflammatories will be detrimental to this process (FYI this is true of any injury, not just ankle sprains).
In the first 48-72 hours of your injury it is recommended to avoid anti inflammatories such as ibuprofen (Nurofen) and Voltaren. This is because the inflammation that occurs is your body’s response to injury and it actually brings special healing cells to the area that are beneficial for your recovery. This includes cells that remove debris and other cells that repair tissue. Therefore this early inflammation is actually a GOOD thing and taking anti inflammatories will be detrimental to this process (FYI this is true of any injury, not just ankle sprains).
The issue is when inflammation persists and essentially the fluid takes up room within your ankle joints and this can cause pressure and therefore additional pain. This is where the above advice for compression and elevation is key and at some stage after the first few days you may need to begin anti inflammatories. This should always be guided by a health care professional as anti inflammatories can commonly cause stomach lining irritation, which is not something to ignore!
If you need help with pain relief it is recommended to speak with your pharmacist or local Shepparton GP, however most people tolerate paracetamol (Panadol) and this has no known negative effect on your healing.
Myth #6: High levels of bruising equals more damage
You may have noticed that everyone bruises to a different degree. For example some people just have to scratch their leg firmly and will bruise while others need a decent hit to bruise. This is related to each person’s clotting and other genetic factors. It can also be related to certain medication for example blood thinners and anti inflammatories can increase the amount of bleeding around an area and therefore the amount fo bruising that comes out. Therefore the amount of bruising that is evident in some ankle sprains doesn’t necessarily mean it is more severe than other injuries where there is minimal bruising. We take into account many factors when diagnosing the severity of the injury, bruising is taken into consideration but there is no hard and fast rule here.

A severe ankle sprain: minimal dark bruising, mostly yellow.

Myth #7: I should rest on the couch and avoid movement
Although when in pain this is what we feel like doing, there is good evidence that early movement will help you to return to normal quicker. When you have sustained a severe injury or you have a lot of swelling you will require periods where you need to elevate your ankle. However if you are able to walk and weightbear this will be helpful. This is where it is important to visit your local Shepparton podiatrist or physiotherapist so we can help you determine what level of rest is required!
Myth #8: Rehab is not worth it, I have gone back to sport before without it
 One of the biggest risk factors for future ankle sprain is previous ankle sprain. While those with mild ankle sprains will likely manage to get back to sport, the issue we commonly see is that the injury has caused a loss of range of motion, strength, balance or coordination on that side. Therefore you can understand how even though you have returned to sport that these deficiencies can result in subsequent ankle sprains and more time away from the sport that you love! With simple assessment and exercises we can get you on track to work on these deficiencies and therefore reduce your risk of future ankle injury!
One of the biggest risk factors for future ankle sprain is previous ankle sprain. While those with mild ankle sprains will likely manage to get back to sport, the issue we commonly see is that the injury has caused a loss of range of motion, strength, balance or coordination on that side. Therefore you can understand how even though you have returned to sport that these deficiencies can result in subsequent ankle sprains and more time away from the sport that you love! With simple assessment and exercises we can get you on track to work on these deficiencies and therefore reduce your risk of future ankle injury!
Myth #9: Ankle braces are better then taping
Both ankle bracing and taping are thought to be just as effective in preventing ankle sprains and are highly recommended for those who have had an ankle injury and are playing sports such as netball, football, basketball, soccer etc. While some are resistant to taping or bracing, when comparing this to lengthy periods out of action should another ankle sprain occur, we know what we would chose!

Ankle braces available at GV Sportscare
The advantages to ankle braces is that you aren’t reliant on the person taping your ankle to tape it correctly or risk of tape cuts or allergic responses to tape (which is more common than you think). If you are paying for your own tape, bracing is also a more economical option as once you have bought 4-5 rolls of tape you have paid for your ankle brace. However football and soccer boots are too narrow for ankle braces so taping is often the only option in these sports. If you wear ankle braces and you are buying new shoes we highly recommend taking your ankle braces with you as you often need 0.5-1 size larger to allow for the ankle brace. We would also advise checking with your Physio or Podiatrist before purchasing an ankle brace as many braces don’t have the metal ‘stays’ built in on the sides and this a crucial component of an ankle brace that will actually prevent injury.
Myth #10: I’ve rolled my ankle more times then I can count, I don’t need to have it assessed
As a netball or footballer you may be one of those people where ~2 sprains/season is a given and you are well versed in your management. We do recommend these are still assessed for a number of reasons:
-recurrent sprains can result in chronic ankle instability, at some stage ankle reconstruction may need to be considered so that you don’t cause irreversible cartilage damage which can lead to osteoarthritis in later life. As we have worked closely with foot and ankle orthopaedic surgeons we can help you decipher when it is time to consider a surgical opinion
-some ankle sprains can result in a ‘high ankle sprain’ which is an injury to the syndesmosis, the joint between to the tibia and fibula. This is a much more serious injury and requires a different management to the average ankle sprain. It can often require surgery to prevent serious ankle instability. Our Shepparton physio and podiatrist can easily screen for this injury with clinical tests
-refer to myth #8, we are experts in finding your deficiencies post injury and providing you with a rehab plan to address this to reduce your risk of re-injury.
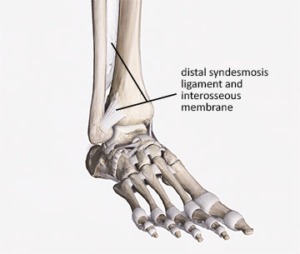
Distal syndesmosis joint = location of high ankle sprain.
Sophie Woodhouse
Physiotherapist Shepparton, GV Sportscare
Tom Davey
Podiatrist Shepparton, GV Sportscare



Image references:
X-ray: https://www.imageinterpretation.co.uk/ankle.php
Calf raise: https://www.popsugar.com.au/fitness/Ankle-Exercises-Do-Avoid-Sprains-Injuries-31086537?utm_medium=redirect&utm_campaign=US:AU&utm_source=www.google.com
Syndesmosis: https://www.academyofclinicalmassage.com/syndesmosis-sprains/
Ankle brace: https://www.djoglobal.com/products/donjoy/donjoy-stabilizing-pro-ankle-brace
Ankle sprain prevention: https://www.facebook.com/watch/?v=948001962331923


 🥩🥗
🥩🥗 



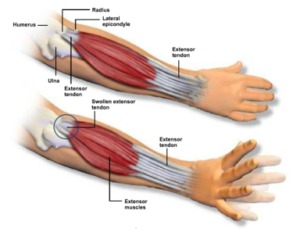






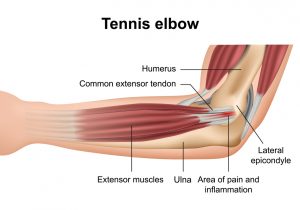 Tendon injuries typically occur when your tendon is unable to adapt to the load you expose it to, often if you train at an intensity that is too high and or there is not enough recovery time after activity before you train again. We also see tendon injuries when a person takes up a new activity or sport for the first time, exposing the tendon to new types of movements and loads or a heavy dose of an activity they don’t normally perform; eg elbow pain resulting from a twice per year gardening project.
Tendon injuries typically occur when your tendon is unable to adapt to the load you expose it to, often if you train at an intensity that is too high and or there is not enough recovery time after activity before you train again. We also see tendon injuries when a person takes up a new activity or sport for the first time, exposing the tendon to new types of movements and loads or a heavy dose of an activity they don’t normally perform; eg elbow pain resulting from a twice per year gardening project.